

Abstract
Introduction: Minimal residual disease (MRD) status reflects depth of response and informs prognosis after first-line therapy in patients (pts) with follicular lymphoma (FL). In the GALLIUM study (NCT01332968), the primary endpoint of investigator (INV)-assessed progression-free survival (PFS) in previously untreated FL pts was significantly improved with obinutuzumab (GA101; G)- versus rituximab (R)-based immunochemotherapy treatment. We previously reported consistently higher MRD response rates with G- versus R-based treatment at the end of induction (EOI) (92% vs 85%, respectively; p=0.0041; Pott et al. ASH 2016). Here we report the correlation of MRD response at EOI with updated PFS data and the results of MRD response assessment during maintenance treatment and follow-up. We also assessed MRD responses and outcome in pts who remained MRD-positive at EOI.
Methods: Previously untreated pts aged ≥18 years with FL requiring treatment were randomized 1:1 to receive 6-8 cycles of G (1000mg IV on days [D] 1, 8, and 15 of cycle [C] 1 and D1 of C2-6 or 8) or R (375mg/m2 IV on D1) plus standard chemotherapy (CHOP, CVP, or bendamustine). Responding pts received the same antibody as maintenance every 2 months for up to 2 years. MRD status was assessed by real-time quantitative (RQ)-PCR assays at mid-induction (MI) in peripheral blood (PB), at EOI in PB and bone marrow, at 4-monthly intervals during maintenance in PB, and at 6-monthly intervals during follow-up in PB, and was defined as negative (MRD response) if RQ-PCR and subsequent nested PCR were negative in all samples analyzed at the respective time point. INV-assessed PFS was estimated using Kaplan-Meier methods (data cut-off, February 12, 2018). Pts were included in the various analyses if they had evaluable MRD data and achieved a complete or partial response at EOI.
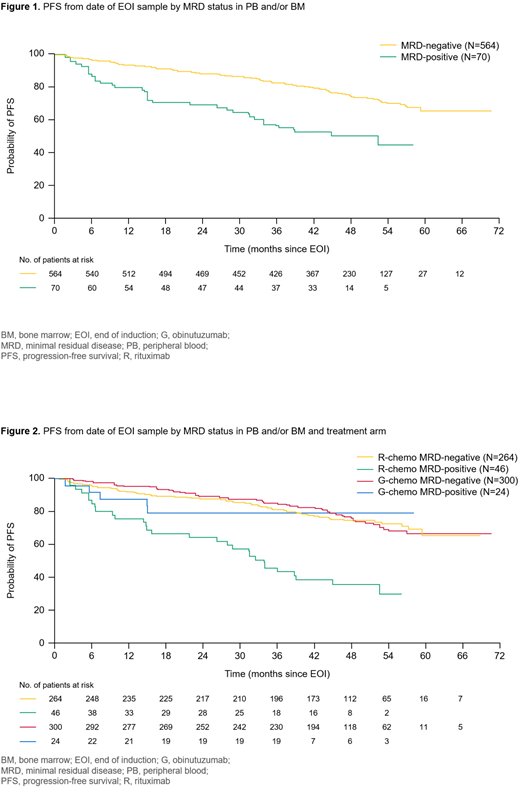
Results: After 57 months' median follow-up, MRD evaluable pts (n=634/1202 randomized FL pts) who had a MRD-negative response at EOI (n=564) continued to have a longer PFS than those who had a MRD-positive response at EOI (n=70; hazard ratio 0.38; 95% confidence interval 0.26, 0.56; p<0.0001; Figure 1), which was irrespective of treatment arm (Figure 2). Of the MRD evaluable pts who continued on maintenance treatment, a MRD-negative response was observed at EOI in 300/324 (92.6%) pts in the G arm versus 264/310 (85.2%) in the R arm (p=0.0034). The majority of the MRD-negative pts remained negative during maintenance. No difference in the MRD relapse rate (conversion to MRD positivity) was observed between pts treated with G or R maintenance (6.3% vs 6.1%, respectively). Two-thirds of MRD-negative responses were sustained throughout the maintenance period (G, 67.0%; R, 63.2%), with a rate of disease progression or death of 11.4% in the G arm and 15.5% in the R arm. Twenty-four pts in the G-chemo arm and 46 pts in the R-chemo arm were MRD positive at EOI but eligible for maintenance treatment based on clinical (CT-based) response. Of these, 22 (92%) pts in the G-chemo arm (18 within the first 4 months of maintenance treatment) and 36 (78%) pts in the R-chemo arm (27 within the first 4 months) achieved MRD negativity during maintenance. Of the 12 pts who never achieved an MRD response, 8 progressed or died within 7 months of EOI, 1 progressed after 15 months, 1 progressed after 26 months, and 2 remained MRD positive during maintenance up to month 8 and month 12, respectively, but had no documented tumor progression until D1348 and D1709.
Conclusions: These data confirm the prognostic value of MRD status at EOI in previously untreated FL pts receiving immunochemotherapy. Analysis of MRD kinetics revealed that most of the pts who achieved MRD negativity at EOI sustained their responses during maintenance. The majority of pts who were MRD positive at EOI achieved MRD negativity during the first 4 months of maintenance. While this is likely to be indicative of the efficacy of continued treatment, it also suggests that response kinetics can be slower than in those pts who have an early MRD response at MI, and that responses that are beyond the sensitivity of the MRD assay may be less deep. Importantly, pts who failed to achieve MRD negativity at EOI or during early maintenance had a high chance of experiencing early progression or death. These data demonstrate the prognostic value of MRD response assessments in previously untreated FL pts receiving immunochemotherapy.
Hoster:F. Hoffman-La Roche: Other: Travel support, Research Funding; Roche Pharma AG: Other: Travel support, Research Funding. Unterhalt:F. Hoffman-La Roche: Other: Travel support. van der Jagt:F. Hoffman-La Roche Ltd: Employment, Honoraria, Research Funding. Janssens:Novartis: Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: Ad board, Speakers Bureau; Amgen: Consultancy, Speakers Bureau; Sanofi-Genzyme: Speakers Bureau; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: Ad board, Speakers Bureau; Janssen: Consultancy, Speakers Bureau. Kneba:Roche: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria. Mayer:Affimed: Research Funding; Roche: Research Funding; Johnson & Johnson: Research Funding; Eisai: Research Funding; Novartis: Research Funding. Pocock:Kent & Canterbury Hospital: Employment. Knapp:Roche: Employment. Danesi:F. Hoffmann-La Roche Ltd: Employment. Nielsen:F. Hoffmann-La Roche Ltd: Employment, Other: Ownership interests PLC. Brown:PAREXEL, external business partner with Roche Products Ltd, Welwyn, UK: Employment. Mundt:Roche: Employment, Other: Ownership interests PLC. Marcus:Gilead: Consultancy; F. Hoffman-La Roche: Other: Travel support and lecture fees; Roche: Consultancy, Other: Travel support and lecture fees . Hiddemann:Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Bayer: Consultancy, Research Funding; F. Hoffman-La Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal